This blog is concurrently posted on Handwriting With Katherine. Check out Katherine for some excellent resources. She is the Handwriting GURU!
As school districts begin to think about transitioning students with disabilities out of school and onto the next phase of life, the idea of becoming as independent or self-sufficient as possible comes to mind. I prefer to use the term self-sufficient as this term implies a sense of power and strength in addition to not requiring assistance from others. At the age of 14 years, school districts are required to begin developing a transition plan. Educators, therapists and parents investigate vocational as well as, social and self-care tasks. In many high schools, Life Skills Programs concentrating on just this effort are charged with the task of fostering self-sufficiency.
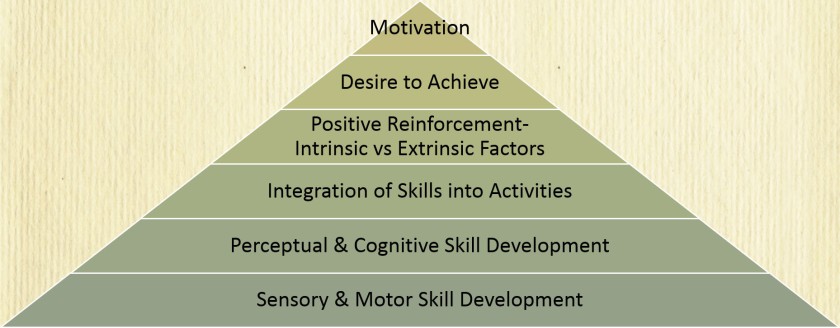
Collectively, we explore both basic [BADLs] and instrumental activities of daily living [IADLs]. BADLs include basic self-care tasks, such as feeding, toileting [including maintaining continence], dressing [donning/doffing and selecting clothes], grooming/bathing, walking and transfers (such as from bed to wheelchair). These are the skills that we have begun to develop since birth. IADLs are more complex skills that we are taught as our thinking skills become more developed and include things like money management, driving/using public transportation, shopping, meal prep, communication using a telephone, computer or tablet, managing medications, housework and basic home maintenance. The IADL and vocational skills are the focus of the Life Skills Programs.
What happens, though, if despite our collective very best efforts, an individual is unable to complete these tasks without some type of assistance? We begin to explore compensatory strategies and levels of assistance that are needed to increase the individual’s ability to become self-sufficient. Assistive technology is a huge area of practice that can be considered and includes both low and high tech devices. Low tech generally means that the strategy or item is simple and generally does not require any type of power source like batteries. Low tech items can include things like a pencil grip or hand-held grabber to a paper calendar or checklist. High tech usually involves a technology device with apps [a computer, cell phone or tablet]. Adaptive technology is another term that is used. Adaptive technology is developed specifically for persons with disabilities and is rarely used by a non-disabled person. Adaptive technology is electronic and includes things like a personal emergency response system [PERS]. A fall detector is a good example of PERS. The purpose of all these technologies is to help the individual develop or maintain their ability to give the individual the power to be independent for as long as possible. Without these technologies, persons with disabilities would be dependent on others to meet many of their needs.
Each and every day, we are challenged with the task of identifying ways for these students to become self-sufficient. There are always budgetary concerns and so we begin with the least restrictive strategy. Let’s use Marty, a life skills student, as an example. Marty is 16 years old and is exploring vocational options. He is enrolled in a retail work experience program through his school with a job coach. We begin to explore his work readiness skills. Is Marty capable of completing all BADL and IADL skills to get him ready to go to and then to get him to work? We look at Marty as he comes to school each day.
Marty comes to school neat and cleanly shaved with hair combed and appears to be well organized. We interview his parents, we may learn some things about Marty that we did not know.
- Is Marty able to prepare for school each morning?
- Can he bathe and dress himself?
- Does he choose his own clothing? Tie his shoes?
- Can he groom himself?
- Can he pack his backpack?
- Make his own lunch or remember to bring money to buy lunch?
- Does he require any sort of assistance?
- If he requires assistance, how much and what type?
- Is there anything that can be done to improve his ability to get ready for school without help from his parents?
Marty is able to shave himself using an electric razor. Initially, he had some difficulty and shaved off part of his eye brows. Marty’s dad worked with him and helped him learn the correct way to shave. He is able to pick out clothing appropriate for the weather but his clothing is not always coordinated in color and patterns. Marty’s mom hangs coordinating clothes on a hanger to help him appear well dressed. It seems that Marty’s parents have many strategies already in hand to deal with his deficits. Marty is able to make his favorite salami sandwich, taking two slices of bread, spreading mustard and adding salami without help. He is able to place and seal his sandwich in a plastic reusable container, add 2 napkins, a cold drink, a piece of fruit and a packaged snack in his insulated lunch bag. Mom checks his backpack before Marty gets on the bus to make sure that he has everything that he needs to get through his day. At the end of the day, Marty is able to empty his backpack and lunch bag. He places the reusable container into the dishwasher and removes any trash that he did not do so when in the cafeteria. All of this shows us that Marty is capable of following a well-established routine with just supervision.
What about taking on new and variable tasks, like those required for his work experience program? In his retail work experience, Marty has a number of tasks to complete on any one day. He needs to take inventory, stock shelves with new merchandise, re-stock shelves when merchandise is sold, organize that merchandise [i.e., matching pairs of shoes in color, size and style] and decide which merchandise needs to be returned. Can Marty perform all these tasks with just a verbal directive? Can he remember the steps to each task? Can he remember when to take lunch? Can he focus on each of the tasks and complete each, meeting the demands of his job? We explore his abilities and begin to develop strategies beginning with the least restrictive.
- Completing job tasks with without supervision requiring only simple verbal directives and a demonstration
- Use a checklist to complete tasks
- Use distant supervision, requiring only someone to monitor his job performance from a distance?
- Use close supervision, requiring someone working in the same area and prompt him to follow his checklist and to complete tasks
Once we get to the level of close supervision, we look at how many tasks is Marty capable of completing? How much of the task is he capable of completing? Does he need to focus on only one task at a time? For example, does Marty need to focus on only matching pairs of shoes and then go back to put the shoes in the correct location?
Here is where we begin to look at low tech strategies. Will a checklist work? Will picture prompts work? Should Marty be partnered with another worker in the store? Finally, we may arrive at high tech solutions, such as needing a tablet with a picture schedule and video modelling to help Marty complete his work with the least amount of assistance from another worker or job coach. At this point, we need to collect data on what Marty is capable of doing, how much assistance is required and what supports have been put in place and failed to get us to the determination that a device is warranted.
Hopefully, at this point, everyone is also focusing on Marty’s abilities to complete IADL skills.
- Is he capable of handling money? Can he create a shopping list? Does he know what a recipe is? Can he differentiate a recipe from a shopping list and can he develop a shopping list by looking at the recipe, determine what he already has in the pantry or refrigerator and what he needs?
- Does Marty take medication? Is Marty able to remember what medication he takes and when he needs to take it consistently? Does Marty know when he needs to order new medication? Does he know when he has to return to the doctor to get a new prescription? Can Marty keep track of his doctor’s appointments? Can he arrange transportation to get to the doctor’s office? Does Marty need a medication reminder?
- Is Marty capable of making plans to organize his schedule? Does he know when others are available to drive him or accompany him on public transportation? Is Marty capable of using a cell phone and Google to navigate from one location to the next? Does Marty need to review a family or group schedule to figure out if, when and who is available to help him?
Many of the questions asked above can be addressed using simple, free or low cost and easily available apps that are available on either Apple or Android devices. Highly structure training and data collection is required to determine if Marty will be capable of using this technology to become self-sufficient. If it were not for technology, Marty may be dependent on others for all his needs and be independent in none.
For more information, please feel free to contact me.
40.823710
-73.398731




 It is difficult for some students to get through school well organized. Parents, teacher and even students become frustrated with missing homework assignments, notes out of order torn or even missing altogether. When frustration ensues, it is easy to become argumentative, which is counter-productive to getting work done.
It is difficult for some students to get through school well organized. Parents, teacher and even students become frustrated with missing homework assignments, notes out of order torn or even missing altogether. When frustration ensues, it is easy to become argumentative, which is counter-productive to getting work done.













 Developing a rapport between client and therapist in which the individuals grow to like one another and experience each other as generally warm, respectful and understanding. Personally, I am not trying to win any popularity contest. I don’t need my clients to ‘like’ me or ‘love’ me. I do need to present myself as someone who will empathize with them and provide them good services.
Developing a rapport between client and therapist in which the individuals grow to like one another and experience each other as generally warm, respectful and understanding. Personally, I am not trying to win any popularity contest. I don’t need my clients to ‘like’ me or ‘love’ me. I do need to present myself as someone who will empathize with them and provide them good services.



































You must be logged in to post a comment.